Plan-Do-Study-Act. Is it a task or test? Learn how to approach PDSA effectively.


“Is it a task or test?” |
Bob Lloyd’s question lives in my head whenever I read PDSAs in slide presentations or articles. Bob has been a significant influence on my Quality Journey — mentor, inspirer, and someone I consider a friend — and his question still does more useful work in five words than most checklists to highlight the essence of PDSA.
I’ve been thinking about it again this week. I spent three days at our Improvement Specialist Program workshop, where each morning began with participants presenting the projects they’re supporting. The problems they choose, and the change ideas they bring, are genuinely interesting. So is the recurring theme that shows up in their PDSAs — and in much of the published Quality Improvement literature alongside them.
There’s too much doing, and not enough testing.
How do we PDSA
Plan-Do-Study-Act (PDSA) is the fundamental methodology for testing a change idea scientifically. Much has been written about its origins and evolution. I’ll sidestep that debate — see the references for the history. The thing that matters is applying the method appropriately.
Task or test?
Most often, PDSAs I see list a task. Send the survey. Implement the new form. Roll out the policy. Even when it isn’t an obvious task, it is still hard to see what the PDSA is testing.
That is why Bob’s question is so useful. Hold each PDSA up to it. If you can answer “test” with a prediction, you have a PDSA. If the honest answer is “task”, what you have is a to-do item with a fancy label under the guise of PDSA.
Cycling off the ramp
PDSA cycles are usually drawn as a ramp. After the first cycle of testing a specific change idea, the second cycle iterates based on the learning from the first. Same change idea, refined — unless the team decides to abandon it and move on to a different one, another ramp.
What I see frequently is that the second, third and fourth cycles on a so-called ramp are different change ideas. Those are not later cycles. They are different PDSA ramps that happen to be stacked together.
Cycles spiral
In reality a PDSA cycle behaves more like a spiral than a ramp. Each cycle’s prediction is shaped by the previous cycle’s learning. You are not just climbing higher on the same staircase; the staircase itself bends as you go, because what you now know about the change idea is different from what you knew at the start.
A spiral is harder to draw on a slide than a ramp, which is probably why the ramp metaphor stuck. But the spiral is the truer picture, and it is the picture worth holding in your head when you write up cycle two.
Ask: what did cycle one teach me, and how does that change my prediction this time? If your cycle-two prediction is identical to cycle one, you probably haven’t learnt anything from cycle one — or you haven’t let what you learnt change what you do next.
What to do instead
Two things, mostly.
1. Test one change idea at a time. Spiral up that ramp until you have enough confidence the change idea leads to an improvement. If it doesn’t, abandon it and start a new ramp on the next change idea. Testing several change ideas in parallel makes the contribution of each impossible to read — one might be cancelling out the other, and you won’t know. (There is a methodology that allows parallel testing of multiple change ideas. It’s called Design of Experiments, or Planned Experimentation, and it’s an advanced approach. Don’t reach for it on cycle one.)
2. Start small. One person. One shift. One department. One machine. One patient. From there, the next cycle takes what you learnt and tests the same change idea on a slightly wider footing — another person, then two, then a shift. Each cycle builds your confidence the change idea will hold up under a wider range of conditions.
A warning about verbs
If the verb in your PDSA aim is one of these, stop and look again:
implement · train · create · survey · perform · roll out · deliver |
Those are task verbs. They describe what you intend to do, not what you intend to test.
A classic example: a PDSA whose aim is “deliver training”. What is the test in that PDSA? Usually nothing — the training is the test, the do, the study and the act all rolled into one event, with no prediction build learning on. Resist the temptation to dress a solution as a PDSA.
PDSA Simulation: spiralling to readiness, then a new ramp
To make this concrete, let me run the training example through to its logical conclusion. The first ramp spirals one change idea — train staff using a slide deck — through four cycles to a deck that’s ready to roll into the standing training programme. The second ramp picks up a different change idea on its own ramp, the way it should. I’ll keep the clinical setting deliberately ordinary so the method, not the topic, is what stands out.
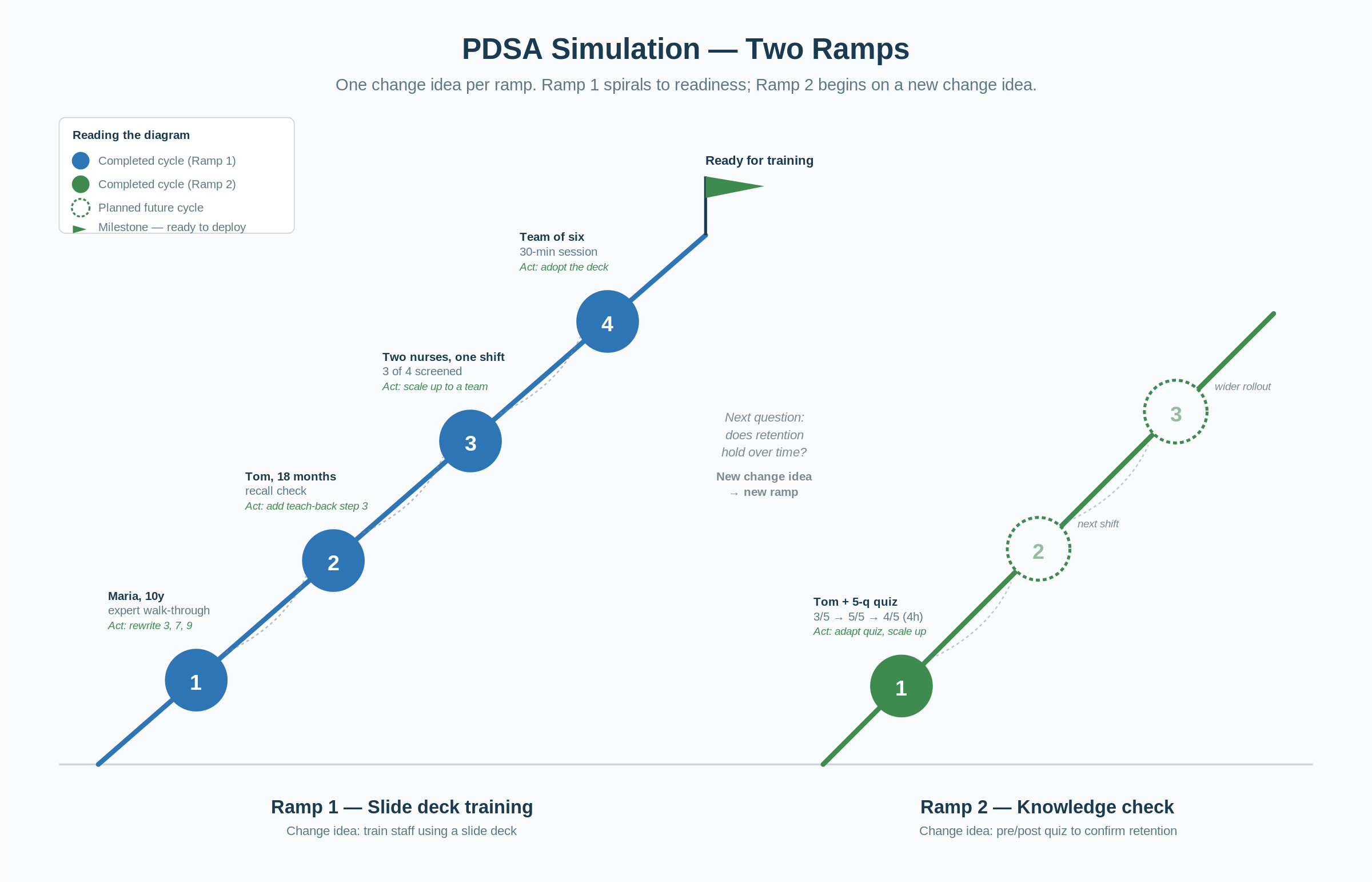
Figure 1. Two ramps. Ramp 1 spirals four cycles on the slide deck to readiness. Ramp 2 begins on a different change idea — a knowledge check — rather than being tacked on as a fifth cycle.
The setting
The improvement project aims to reduce the delay to first antibiotic dose for adult patients presenting with suspected sepsis in the Emergency Department. The team’s driver diagram identifies a new sepsis screening tool, to be completed within 30 minutes of triage, as a key process change. Training is a secondary driver, so let's take this common scenario:
• Outcome measure: time from triage to first antibiotic dose
• Process measure: percentage of eligible admissions with the screening tool completed within 30 minutes
• Theory: if staff reliably use the new screening tool, the antibiotic delay will fall
• First change idea (Ramp 1): train staff on the new tool using a slide deck
• Second change idea (Ramp 2, picked up later): add a pre/post knowledge check to confirm retention over time
Notice what we are not doing: we’re not running training as the PDSA (as often happens). The training is the change idea. Each PDSA cycle tests whether that change idea — in its current form and based on iterative learning — is fit to roll into actual training sessions.
Ramp 1 — slide deck testing
Cycle 1: one experienced nurse, one quiet morning
Plan. I’ll sit with Maria, a senior ED nurse with ten years’ experience, and walk her through the draft 12-slide deck. She knows the existing process well, so any confusion will tell me the slides themselves are unclear, not the process.
Predict. Maria will follow the flow, but will flag at least one or two slides where the wording or sequence doesn’t match how things really run in the department.
Do. Twenty minutes on a Tuesday before her shift. I read the slides; she talked back at me.
Study. Maria stalled on slide 3 (an acronym she’d never heard) and slide 7 (the decision flow skipped a branch). The case example on slide 9 was, in her words, nothing like a real ED arrival. Prediction partially confirmed — she did flag issues, but more than I expected, and one of them was structural.
Act. Adapt. Rewrite slides 3 and 7, replace the case example with one Maria helped me sketch. Move up the ramp.
Cycle 2: one less-experienced nurse, the next day
Plan. Same revised deck, walked through with Tom, eighteen months in the department. If the revisions hold, Tom should follow without stalling and be able to describe the screening steps when I check back later.
Predict. Tom will follow without questions and will recall the steps five minutes later.
Do. Walked through the deck before Tom started his shift.
Study. No stalls during the walk-through. Five minutes later, asked him to describe the screening steps in his own words. He got steps 1, 2, 4 and 5. Step 3 — the one we’d just rewritten — he couldn’t reproduce. He said the slides had made sense in the moment.
Act. Adapt the deck again. Step 3 is sticky in conversation but slippery in recall, so add a teach-back prompt at that point in the deck — the trainer pauses, the learner says it back. Same change idea, refined.
Cycle 3: two nurses, one shift
Plan. Run the deck (now with the teach-back on step 3) with two nurses at the start of a shift, then track the process measure for that shift.
Predict. Both nurses will describe the steps immediately after training and at end of shift, and the screening tool will be completed within 30 minutes for most eligible admissions on that shift.
Do. Trained two nurses Wednesday morning. Pulled the screening tool data at the end of shift.
Study. Both nurses described the steps cleanly after training, and again at end of shift — including step 3. The tool was completed within 30 minutes for three of four eligible admissions. The process measure moved.
Act. The deck holds up with two people, walked through one-on-one. Next test: does it still work when delivered as a single group session, the way it will actually be used?
Cycle 4: a team of six, one 30-minute session
Plan. Deliver the deck as a single 30-minute training session to a team of six nurses on Friday morning, in the same format the standing training programme will use. Track the process measure on the shifts those nurses work over the next two days.
Predict. The session will run to time, all six will describe the steps cleanly afterwards, and the screening tool will be completed within 30 minutes for the majority of eligible admissions on their shifts.
Do. Ran the 30-minute session Friday morning. Six nurses, one trainer, the deck as it now stands. Followed up over Saturday and Sunday shifts.
Study. Session ran to twenty-eight minutes. All six described the steps after, including step 3. Across the two follow-up days, the screening tool was completed within 30 minutes for sixteen of twenty eligible admissions — the process measure now sits where the team needs it at this stage (we are not implementing yet).
Act. Adopt. The deck, as it now reads, is ready to roll into the standing training programme. The next PDSA picks up a different question — does retention hold over time? — and that question is a new change idea on its own ramp.
Ramp 2 — knowledge check
With the deck adopted, the team turns to a different question. The deck gets staff using the screening tool today; what about three weeks from now, when the training session is a fading memory? Does a knowledge check bolster use of the screening tool? That’s a different change idea — a short pre- and post-training knowledge check, designed to surface gaps and force a second pass on weak areas — and it deserves its own ramp, not a fifth cycle bolted onto the first.
Cycle 1: one nurse, one short quiz
Plan. Build a five-question pre/post quiz tied to the screening tool’s steps. Run it with Tom, who already has the slide-deck version of the training, so we’re isolating what the quiz adds.
Predict. Tom will score higher post- than pre-, will identify step 3 as his weak area, and will retain it for at least four hours.
Do. Tom completed the pre-quiz (3 out of 5, missed step 3 and step 5), did the slide deck again, then the post-quiz (5 out of 5). I checked back four hours into his shift with the same questions: 4 out of 5.
Study. The quiz did what I hoped at the front end — flagged step 3 cleanly and gave the training something specific to reinforce. Four-hour retention is better than what we saw without the quiz, but step 5 slipped, which I hadn’t predicted. Question 2 also confused him; he said it could be read two ways.
Act. Adapt the quiz. Reword question 2. Add a sixth question built around a short clinical vignette to test application rather than recall. Plan the next cycle with two nurses on the next shift, and start tracking whether retention at one and three weeks holds up as more staff move through the new training format.
What this simulation is meant to show
Three things, really. On Ramp 1, each cycle tested one specific thing and produced learning that shaped the next — the cycle-two prediction was different from cycle one, and the cycle-three prediction was different again. The change idea didn’t change; the deck did. We got to readiness with evidence rather than a hopeful rollout.
Then, when a genuinely different question came along — does retention hold over time? — we treated it as a different change idea and put it on its own ramp, rather than quietly relabelling cycle five as more of the same. That’s what cycling — or spiralling — through PDSA looks like when it’s done as a test rather than a task.
Before your next cycle
So when you sit down to plan your next cycle, ask Bob’s question first. Is this a task or a test? Then write your prediction down before you do anything else. If you can be wrong about it, you’re doing PDSA. If you can’t, you’re doing too much doing and not enough planning.
Build your habit by using a PDSA template (see the IHI PDSA worksheet here). Practise with this structure until it becomes second nature, and then keep using it (like a martial arts kata).
References
- Moen, R., Nolan, T. & Provost, L. Quality Improvement Through Planned Experimentation (3rd ed.). McGraw-Hill, 2012. The standard reference for testing multiple change ideas in parallel.
- Provost, L. & Murray, S. The Health Care Data Guide: Learning from Data for Improvement. Jossey-Bass, 2011. A useful companion on the measurement that supports PDSA cycles.
- Langley, G., Moen, R., Nolan, K., Nolan, T., Norman, C. & Provost, L. The Improvement Guide (2nd ed.). Jossey-Bass, 2009. The model for improvement and the original modern PDSA framing.
- Moen, R.D. & Norman, C.L. (2010). Circling Back: Clearing up myths about the Deming cycle and seeing how it keeps evolving. Quality Progress, 43(11), 22–28. The single most-cited piece on the evolution. Tracks the cycle from Shewhart through Deming, the Japanese adaptation, and back. Available via ASQ and frequently mirrored on the Deming Institute site.
- Moen, R.D. (2009). Foundation and History of the PDSA Cycle. Paper presented at the Asian Network for Quality Conference, Tokyo. The longer, more academic version of the same argument; the Deming Institute hosts the PDF.
Other helpful information
- Robert (Bob) Lloyd was the Vice President of Improvement Capability at the Institute for Healthcare Improvement and a longstanding teacher of improvement methods (now in 'preferment').
- The Institute for Healthcare Improvement (IHI) is a global non-profit that has shaped much of the modern QI vocabulary. Learn more about the Institute for Healthcare Improvement.